
GoodLife. Live it Well was an exciting aspirational campaign that promoted good health and positive lifestyles among Ghanaians. By asking, “What is Your Good Life?”, the national initiative encouraged self-reflection while linking personal happiness to the practice of healthy behaviors.
Health messages moved beyond instructive commands and capitalized on personal experiences that engaged Ghanaians on issues relevant to their daily lives. This was achieved through the use of innovative, entertaining and educational mass media, including: a highly rated television game show, a reality-based radio magazine, cell phone partnerships and community outreach tools.
GoodLife, which ran from 2009-2014, was a unifying umbrella brand implemented under the Ghana Behavior Change Support (BCS) Project. BCS sought to increase demand and use of commodities and services as well as positive behaviors related to six key health areas: family planning, malaria, maternal and child health, nutrition, water and sanitation and HIV (the latter through a special activity with the Ghana Police Service). The project was managed by the Johns Hopkins Center for Communication Programs (CCP) in partnership with the Ministry of Health and the Ghana Health Service (GHS).
Watch a video describing the campaign!
Timeline
Inquire
Before the launch of the campaign, the team carefullly reviewed existing data and surveys. Several trends emerged from the 2008 Ghana Demographic and Health Survey and Ghana Maternal Health Survey (GMHS) 2007, both released in 2009. Several indicators had substantially improved (exclusive breastfeeding, ITN use); others had remained largely stagnant (e.g. infant and under five mortality, anemia); and, some had unfortunately worsened (contraceptive use, maternal mortality).
A summary of the key findings includes:
- Family planning/reproductive health. In a country that had historically seen a steady increase in the use of family planning, new data revealed that this trend had reversed with a drop in modern contraceptive use from 19% to 17% between 2003 and 2008. During this same period, the total fertility rate dropped from 4.4 to 4.0 per woman (GDHS, 2009).
- Maternal mortality. The overall morbidity and mortality rate (MMR) of 580 deaths per 100,000 live births was substantially higher than previous estimates. The major causes of maternal deaths cited were: 24% hemorrhage, 11% abortion, 9% hypertension, and 7% sepsis, with over 40% unspecified as “other” (GMHS, 2009).
- Infant and under five mortality. The infant mortality rate had largely stagnated since 1993 (GDHS, 2009), only achieving marginal if any reductions during this period. More than half of the deaths in Ghana each year were among children under five, with neonatal mortality increasing as a proportion of childhood deaths.
- Malaria. Although there was a huge increase in ITN ownership from 3% in 2003 to 33% in 2008, there was still a gap in net ownership and use. Approximately 28% of children and 20% of pregnant women slept under an ITN. At the time of the survey, only 40% of pregnant women received IPTp during antenatal visit to prevent malaria during pregnancy (GDHS, 2009).
Design the Strategy
The BCS Project employed a Communication for Social Change Model (see image below), blending community, interpersonal, and mass media approaches to integrate the four program elements: behavior change communication (BCC); community mobilization; systems strengthening and capacity building.

The Communication for Social Change approach is an iterative process where “community dialogue” and “collective action” work together to produce social change in a community to improve the health and welfare of all its members. As part of the strategy development process, BCS fostered partnerships among key stakeholders, including the Ghana Health Service/Family Health Division, USAID, UNFPA and key program implementers.
The goal of the strategy was for the GoodLife concept to unite all activities and media, maintaining the GoodLife brand as the centerpiece of the campaign. More specifically, the strategy provided a mechanism that:
- Developed an overarching, unifying concept that made health messaging personally relevant;
- Ensured coherence and continuity to health communication activities in order to minimize potential confusion between different types of health messages that would be promoted over the course of the project;
- Prompted the desire to learn more about disease prevention and health promotion and laid the foundation for individuals to adopt a variety of preventive and behavioral actions that the project promoted;
- Avoided message fatigue and confusion among the audience as the campaign promoted messages on each health topic;
- Placed the individual and what they wanted at the center of health messaging, which clearly linked something everyone wants (a good life) to health.
Through a socio-ecological lens, the campaign strategy was implemented at the national, regional, and community levels through mutually reinforcing approaches that were used for BCC activities, including:
- Integrated Approaches that addressed a wide spectrum of topics simultaneously over a prolonged period;
- Health Campaigns and Approaches that focused on one or two specific health issues at a time using multi-media at high intensity for limited duration;
- Regional District and Communication Activations events that reinforced the on-going media and community mobilization activities.
Mass media activities had a national reach. District and community-level activities were implemented in three regions of Ghana: Greater Accra, Central and Western, covering about one-third of the population.
Create and Test
In order to meet deadlines and maintain quality outputs, the BCS team realized it needed multiple creative partners. The project used a competitive bidding process to identify three local qualified agencies to take on different aspects of the campaign. Of the three companies selected, one was designated to work specifically on the central GoodLife materials.
During Year 1, the concept of “Good Life. Live It Well “ was developed and pre-tested. The concept and its link to health were universally well received and understood during pre-testing. A logo [shown here] was developed based on an adinkra symbol, maximizing the link to Ghanaian culture and history. The logo was modern and appealing, but at the same time, played on the traditional symbol “Nkyemekyeme,” that signifies initiative, creativity and determination can help one overcome obstacles in life.
Also during Year 1, six Ghanaians representing a cross-section of the country’s population were selected to tell personal stories about what they value in life—in other words their “Good Life”—and how health enabled them to achieve their good life. Their testimonies were developed for television, radio and print.
A song produced for the brand was extremely popular with the pre-test audience. In addition to the television and radio materials, posters, flyers, print ads, web banners, t-shirts, billboards and a music video were also developed to promote the GoodLife brand. Various web-based and social media channels (e.g. Facebook, Twitter, YouTube) were also used to extend the GoodLife platform.
Mobilize and Monitor
The campaign was rolled out in two phases:
During Phase 1:
- A Teaser segment, aimed to stimulate curiosity about the campaign, ran from October-November 2010. This segment consisted of TV and Radio spots, newspaper ads, posters, community events, and SMS messaging that were not linked to a health issue.
- A Brand Positioning segment ran from December 2010 to May 2011. This segment revealed the brand’s link to health issues and to GHS. It was promoted through the use of TV, radio, billboards, posters, and T- shirts.
- A Brand Establishment segment was designed to increase visibility and understanding of the campaign. This segment involved a music concert held in January 2011 as well as a GoodLife Quiz in newspapers, a theme song and music video.
During Phase 2:
- The Maintain the Brand segment included increasing visibility of the brand by outfitting community volunteers with GoodLife vests, making sure that all community materials had a GoodLife logo and slogan, and weaving GoodLife themes into community dialogue guides.
- GoodLife Media Platforms included on-going shows that drew a regular audience and addressed a variety of health topics via a weekly radio show, and the GoodLife TV Game Show.
- Mass Media Campaigns were used to link GoodLife to all Ghana Health Service campaigns by adding the GoodLife logo and phrase to the campaign slogan.
National Mass Media Campaigns
BCS implemented intensive national mass media campaigns. Below are links to materials produced by some of the campaigns:
- Family planning
- Malaria
- Nutrition
- Overall GoodLife initiative – see list below “Resources”
More than 120 video and radio spots and documentaries were produced in English, and in some cases, up to eight Ghanaian languages. Collectively, these spots aired more than 100,000 times.
Monitoring
BCS developed a robust monitoring system aligned with the project’s key BCC strategies. The monitoring platform tracked outputs at the community level and in the media, collected service statistics data when available, and conducted periodic survey research as well as data quality assessments.

“I have really benefited from being a community mobilizer; God bless USAID for the BCS project.”
-Eunice Aidoo, Community Mobilizer

Campaign workers distributing GoodLife materials as part of the teaser phase of the campaign.
- Ghana BCS Media Materials Inventory
- What is Your Good Life?
- GoodLife Ghana Activity Cards
- GoodLife Ghana Theme Videos
- GoodLife Ghana Game Show
- Life is What You Make It – Theme Song for GoodLife Ghana
- GoodLife Teaser Buzz Card
- GoodLife TV Quizzes
- GoodLife Live it Well Quiz
- Goodlife Live it Well Posters
- GoodLife Ghana T-Shirts
- Kwame & Friends: Fun with Community Mobilization
- Community Action Kit Health Information Cards
- BCS Program Monitoring Form
Evaluate and Evolve
BCS used a rigorous and comprehensive approach to evaluate program activities and derive valid and reliable data for program management of both outputs and outcomes. A baseline, midpoint omnibus, and endline survey assessment were conducted during project implementation to evaluate the effect of the campaigns and identify innovative approaches that were beneficial to the strategic decisions-making process. The endline survey interviewed respondents from 1,942 households in 98 enumeration areas and assessed the impact of the project in regards to behavioral changes from baseline and comparisons between groups exposed and unexposed to different media messages and strategies.
Much of the results showed significant improvements over estimates derived from national surveys, including the 2008-2009 Ghana Demographic Health Survey, the Ghana Multiple Indicator Cluster Survey (2010) and the Ghana Maternal Health Survey (2010). Results of the evaluation of campaign activities showed increases in desired indicators as well as significant associations between positive health behaviors and exposure to BCS campaigns.
Campaign reach and recall
The BCS campaigns achieved good reach in the community for all health focus areas. Campaigns on FP promotion and malaria prevention received the highest exposure compared to other health areas: 91% of all the study participants reported exposure to the project’s FP campaign and 81% of participants had been exposed to the malaria prevention campaign. Nearly a third of participants (74%) had been exposed to the nutrition campaign, 70% to the GoodLIfe campaign and more than half (58%) to the campaign promoting oral rehydration salts and zinc (ORS/Zinc) for the treatment of childhood diarrhea.
Impact
Child Health
- Sale of zinc tablets increased 280% after media campaign
Nutrition
- The proportion of women who immediately started breastfeeding within 30 minutes of birth increased significantly in Western and Central regions, but not in Greater Accra (please see chart).
Malaria
- 80% of pregnant women in rural areas exposed to GoodLife slept under bed nets, compared to 36% of those not exposed
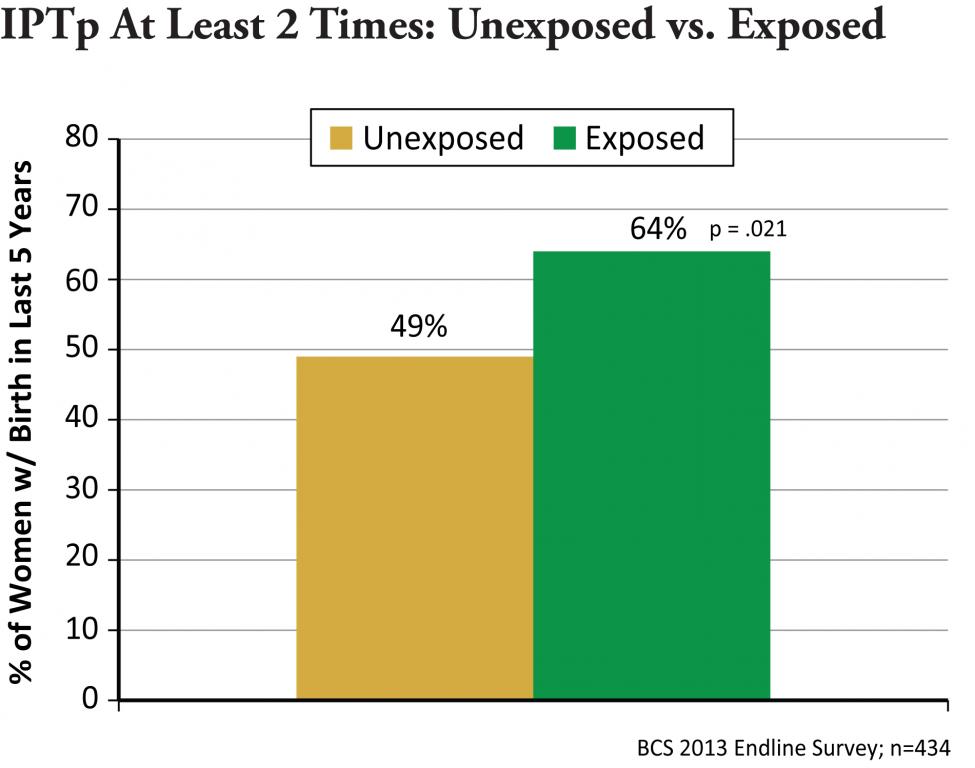
- Women exposed (64%) to the GoodLife malaria messages were significantly more likely to have taken at least two doses of IPTp while they were pregnant compared to those unexposed (49%)
Maternal Health
- There was a 47% increase in blood donations in the Greater Accra Region after the start of GoodLife social mobilization and blood drives. About half of all maternal deaths in the region are due to postpartum hemorrhage and lack of available blood.
- The proportion of females who received a post-partum checkup from health personnel increased from 79% at Baseline to 87% at Endline (p<.001).
Family Planning
- Contraceptive prevalence increased from 17 to 23% between 2008 and 2011
- In the endline survey, 18% of the none/low exposed used a modern FP method, as compared to 20 and 23% of the medium and high exposed, respectively.

Handwashing
- Exposure to GoodLife handwashing messages had a positive impact on
- handwashing behaviors before eating (41% of exposed vs. 32% of unexposed) and before food preparation (15% of exposed vs. 8% of unexposed).
Cost benefit
- The campaign achieved its goals for an average of 3 cents per person for the mass media activities and 38 cents per person for the community mobilization activities
Lessons Learned
One important lesson is that program activities and capacity building are mutually enhancing and deserve equal attention as a strategy for long-term sustainability. Specifically, capacity building without intensive program implementation is futile, as the individuals and institutions that are strengthened do not have opportunities to apply and practice their enhanced capacity in a mentored environment. It is also important that health outcomes continue to be improved; therefore, the support of intensive program activities during the process of capacity building is critical.
Date of Publication: April 20, 2022


